Benzodiazepine Addiction in Elderly Patients: What Families Should Know
Benzodiazepine addiction in elderly patients is more common than families realize. Learn the warning signs, risks, and safe steps to help your aging loved one.

Benzodiazepine addiction in elderly patients is one of the most underrecognized public health problems in geriatric medicine today. These medications, which include widely prescribed drugs like Valium, Ativan, Klonopin, and Xanax, are handed out regularly for anxiety, insomnia, and muscle tension. The problem is that for older adults, what starts as a legitimate prescription can quietly become a dependency that looks nothing like what most families imagine when they hear the word “addiction.”
There is no stereotype that fits here. A 72-year-old retired teacher taking Ativan every night for sleep looks very different from what most people picture as a substance use problem. That is exactly why it goes unnoticed for so long.
The consequences, though, are serious. Long-term benzodiazepine use in older adults is linked to a significantly higher risk of falls and fractures, memory loss, confusion, delirium, and an increased likelihood of developing dementia. According to research published in peer-reviewed geriatric journals, benzodiazepines are among the most inappropriately prescribed drug classes for the elderly population, and only about one-third of prescriptions in this age group are considered clinically appropriate.
This article is written for families who want to understand what is actually happening when an aging parent or grandparent has been taking these medications for months or years. You will learn how dependence develops, what warning signs to look for, what the real risks are, and how to work with doctors to find safer alternatives or taper off safely.
What Are Benzodiazepines and Why Are They So Commonly Prescribed to Older Adults?
Benzodiazepines are a class of central nervous system depressants that work by enhancing the effect of a neurotransmitter called gamma-aminobutyric acid, or GABA. The result is a calming, sedating effect on the brain. They are effective in the short term. The issue is that “short term” in clinical guidelines typically means two to four weeks, and many older adults end up taking them for years.
Doctors prescribe these drugs to seniors for several common reasons:
- Generalized anxiety disorder (GAD)
- Insomnia and sleep disorders
- Muscle spasms and tension
- Panic disorder
- Seizure disorders
- Alcohol withdrawal management
Some of the most common benzodiazepines prescribed to elderly patients include:


- Lorazepam (Ativan)
- Alprazolam (Xanax)
- Diazepam (Valium)
- Clonazepam (Klonopin)
- Temazepam (Restoril)
- Oxazepam (Serax)
The challenge is that older adults are not the same as younger adults physiologically. Their bodies process medications differently. Liver function slows, kidney clearance decreases, and body fat distribution shifts. This means benzodiazepines stay in the system longer, accumulate more easily, and produce stronger sedative effects at the same dose that would be unremarkable in a 35-year-old.
Benzodiazepines with oxidative metabolic pathways and longer half-lives, such as diazepam and flurazepam, are particularly likely to accumulate in the bodies of older patients, causing prolonged sedation and increased risk of adverse effects.
How Benzodiazepine Dependence Develops in Elderly Patients
The Difference Between Dependence and Addiction
This is a distinction that matters, and families often get confused by the language. Physical dependence means the body has adapted to the presence of the drug and will produce withdrawal symptoms if it is stopped or reduced. Addiction involves compulsive use despite harm, often with drug-seeking behavior.
Older adults, like all benzodiazepine patients, are vulnerable to developing physical dependence through long-term prescriptions, and long-term use is defined as daily use lasting more than two to four weeks.
Many elderly patients are physically dependent on benzodiazepines without engaging in any classic “drug-seeking” behavior. They take exactly what is prescribed. But when the drug is stopped or reduced, the withdrawal can be intense and difficult, which is why many people stay on it far longer than anyone originally intended.
Why Long-Term Use Happens
Several factors push elderly patients into long-term benzodiazepine use:
- Renewal without reassessment. Prescriptions get refilled at routine visits without a discussion about whether the medication is still needed.
- Tolerance. Over time, the same dose produces less effect, which can lead to dose increases.
- Rebound symptoms. When the drug wears off between doses, the original anxiety or insomnia often returns with greater intensity, convincing the patient that they still need the medication.
- Fear of withdrawal. Both patients and physicians are often reluctant to attempt tapering because of concerns about what will happen when the drug is reduced.
- Polypharmacy complexity. Polypharmacy and comorbidities are major risk factors for benzodiazepine misuse in the elderly.
7 Critical Warning Signs of Benzodiazepine Addiction in Elderly Patients
Families often miss the early signs because the symptoms look like normal aging or unrelated health problems. Here are the seven warning signs to watch closely.
1. Taking Higher Doses Than Prescribed
If your loved one is taking more than the prescribed amount or asking for early refills, this is a red flag. They may report that the medication “just isn’t working the way it used to,” which is a sign that tolerance has developed.
2. Memory Problems and Confusion
The use of benzodiazepines among elderly patients has been associated with cognitive impairment characterized by anterograde amnesia, diminished short-term recall, and increased forgetfulness. If your parent is forgetting conversations that happened just hours ago or seems unusually disoriented, this could be medication-related rather than a new neurological condition.
3. Increased Falls or Near-Falls
Falls are one of the most dangerous consequences of benzodiazepine use in seniors. If your loved one has started tripping, losing balance, or has already had a fall, the medication may be a contributing factor. The 2023 American Geriatrics Society Beers Criteria recommends avoiding benzodiazepines in all older adults due to the risk of cognitive impairment, delirium, falls, fractures, and motor vehicle crashes.
4. Withdrawal Symptoms Between Doses
Watch for tremors, irritability, sweating, or intense anxiety that appears a few hours after the last dose. This is called interdose withdrawal, and it is a sign that physical dependence has formed.
5. Emotional and Behavioral Changes
Increased agitation, mood swings, unusual sadness, or uncharacteristic irritability can all be signs that benzodiazepine dependence is affecting your loved one’s mental state.
6. Asking Multiple Doctors for Prescriptions
While not always the case, some patients with benzodiazepine dependency may visit more than one provider to secure additional prescriptions. This is sometimes called “doctor shopping” and is a more clear-cut marker of addiction beyond physical dependence.
7. Extreme Distress at the Idea of Stopping
Some of the reasons older patients resist reducing benzodiazepine use include fear of a return of anxiety they believe is well-controlled by the drug, a lack of perceived harm, fear of worsening insomnia, and the perceived need for continued access to manage anxiety-provoking social situations. If your loved one becomes highly anxious or upset when a doctor suggests reducing the dose, that reaction itself can be informative.
The Real Risks: What Long-Term Benzodiazepine Use Does to an Elderly Brain and Body
Cognitive Decline and Dementia Risk
This is the risk that gets the most attention in the medical literature, and for good reason. A lifetime use of more than 90 doses of benzodiazepines, equivalent to twice a week for one year, has been shown to confer a 50% higher risk of dementia and to double the risk of death.
The relationship between benzodiazepine use and dementia in the elderly is still being studied, but the signal is strong enough that most major geriatric guidelines now explicitly recommend against prescribing these drugs to older patients unless absolutely necessary.
Falls and Fractures
Hip fractures in elderly patients can be life-altering, and sometimes life-ending. Sedative-hypnotic medications like benzodiazepines impair motor coordination, reaction time, and balance. The risk of hip fracture is greatest within the first two weeks of therapy, and the risk increases with higher doses and when these drugs are combined with other centrally acting medications.
Respiratory Problems
In patients who also have chronic obstructive pulmonary disease (COPD), sleep apnea, or other respiratory conditions, benzodiazepines can dangerously slow breathing, especially during sleep. This becomes even more dangerous when combined with opioid pain medications.
Dangerous Drug Interactions
Older adults are often on multiple medications for heart disease, diabetes, high blood pressure, and other chronic conditions. Dangerous drug interactions are common in seniors because benzodiazepines can interact with other medications, leading to confusion and over-sedation.
Emergency Department Visits
The problem is common enough to be visible in hospital data. A recent study estimated that approximately 212,770 emergency department visits involving adverse medication-related events in 2016 were related to benzodiazepine use, representing roughly 10% of all ED visits attributed to adverse medication-related events.
What the Medical Guidelines Say About Benzodiazepines and Elderly Patients
If your family is looking for validation that your concerns are legitimate, the medical community is squarely on your side here.
The American Geriatrics Society (AGS) Beers Criteria, which is the gold standard set of prescribing guidelines for older adults, explicitly lists benzodiazepines as potentially inappropriate medications for all older adults. The criteria cover both short-acting and long-acting forms. This is not a fringe position — it is the mainstream consensus of geriatric medicine.
The STOPP criteria (Screening Tool of Older Person’s Prescriptions), a parallel European framework, recommends that benzodiazepines not be taken for more than four weeks, and advises that all patients on these drugs for longer than two weeks require a gradual tapering approach because of withdrawal syndrome risk.
The Beers Criteria specifically notes that older adults are more sensitive to benzodiazepines and their bodies do not break down long-acting versions as quickly, raising the risk of cognitive impairment, confusion, falls, and accidents.
If your loved one’s doctor is still prescribing these medications long-term without regular reassessment, it is entirely appropriate to ask for a second opinion from a geriatrician.
How to Talk to an Elderly Parent About Their Benzodiazepine Use
This is genuinely one of the hardest parts for families. Many older adults do not recognize that they have a problem. They see the medication as necessary, not harmful. Approaching this conversation poorly can damage trust and close off the discussion.
Here is a practical approach:
Do:
- Lead with care, not accusation. Start with something like: “I’ve been reading about this medication and I’m worried about some of the risks for people your age.”
- Ask questions more than you make statements. “Have you noticed your memory feeling off lately?” opens a conversation. “You’re addicted to your pills” shuts one down.
- Bring information from reputable sources — your doctor, the American Geriatrics Society guidelines, or materials from SAMHSA’s official resource library.
- Suggest a joint appointment with their physician where you can all discuss the medication review together.
Don’t:
- Threaten or issue ultimatums about the medication.
- Downplay how real the withdrawal fear is. It is legitimate and it needs to be addressed medically, not emotionally.
- Attempt any kind of dose reduction without medical supervision. Stopping benzodiazepines abruptly can cause seizures and is genuinely dangerous.
Benzodiazepine Withdrawal in Elderly Patients: What Families Need to Know
Withdrawal from benzodiazepines is one of the most medically serious withdrawal syndromes. Unlike opioid withdrawal, which is agonizing but rarely fatal, benzodiazepine withdrawal can cause seizures and death if handled abruptly or without supervision.
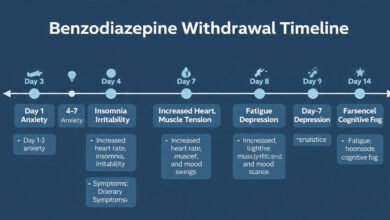
Common Withdrawal Symptoms in Older Adults
- Intense anxiety and panic
- Insomnia that is far worse than before the medication was started
- Tremors and muscle twitching
- Irritability and mood swings
- Sweating and nausea
- Heightened sensory sensitivity (lights seem brighter, sounds seem louder)
- In severe cases: confusion, delirium, or seizures
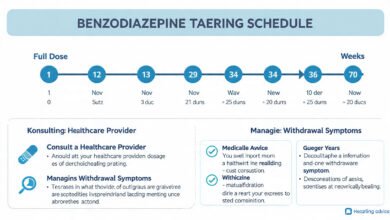
The Gradual Tapering Approach
The standard medical approach to safely discontinuing benzodiazepines in elderly patients involves a slow, individualized taper under physician guidance.
Some authorities recommend tapering the dose by 25% every two weeks; in elderly patients, a longer tapering schedule over four to five months is generally preferred, and withdrawal symptoms tend to be most severe during the last quarter of the taper.
The good news is that the outcomes are better than most families (and many doctors) expect. Contrary to most clinicians’ belief, discontinuation of chronic benzodiazepine use in elderly patients is feasible with adequate psychotherapeutic or pharmacological strategies, and can lead to long-term abstinence.
Even simple interventions work. In the EMPOWER trial, within six months of receiving an educational brochure about sedative-hypnotic risks along with a tapering guide, 27% of elderly participants completely discontinued benzodiazepine use compared with only 5% in the control group.
Safe Alternatives to Benzodiazepines for Anxiety and Insomnia in Older Adults
One reason elderly patients and their families are reluctant to push back on benzodiazepine prescriptions is a legitimate question: “If we stop this, what replaces it?” The good news is that there are effective alternatives for both anxiety and insomnia.
For Anxiety
- SSRIs and SNRIs (such as sertraline or venlafaxine) are considered first-line treatments for generalized anxiety disorder in older adults and do not carry the same dependency or cognitive risks.
- Buspirone, an anti-anxiety medication that is non-habit-forming, is another option for chronic anxiety management.
- Cognitive Behavioral Therapy (CBT) has strong evidence for treating anxiety and does not require any medication at all. It addresses the root thought patterns that drive anxiety rather than simply suppressing the physiological response.
For Insomnia
- Cognitive Behavioral Therapy for Insomnia (CBT-I) is now considered the first-line treatment for chronic insomnia in all adults, including the elderly. It consistently outperforms medication in long-term follow-up studies.
- Melatonin in low doses can be helpful for sleep maintenance issues in older adults.
- Sleep hygiene improvements — consistent sleep schedules, reduced screen time, limiting caffeine after noon, keeping the bedroom cool and dark — may seem basic but have real clinical impact.
- Doxepin at very low doses (3–6 mg) has FDA approval for insomnia and is considered safer for elderly patients than benzodiazepines.
For families seeking detailed guidance on evidence-based treatment options, the National Institute on Aging’s health resources offer extensive, plain-language information on medication safety for older adults.
How Families Can Support Recovery and Deprescribing
Deprescribing is the formal term for the supervised, intentional process of reducing and stopping a medication that is no longer benefiting the patient. For benzodiazepines in elderly patients, deprescribing has become a priority across geriatric medicine.
Here is how families can actively support this process:
Build a Medication List
Write down every medication your loved one takes, including over-the-counter drugs and supplements. Bring this to every doctor’s appointment. This helps physicians identify dangerous interactions and spot redundancies.
Advocate for Medication Reviews
Ask their primary care physician for a formal medication review at least once a year. Many older adults have medications that were started by one doctor, renewed by another, and never reassessed by either.
Create a Support Structure During Tapering
The tapering process takes months, not weeks, and it is emotionally demanding. Being present, checking in regularly, and reducing sources of stress at home during this period significantly improves outcomes.
Connect with a Geriatric Specialist
Not all treatment centers specialize in senior-specific addiction care, so finding a facility or physician with expertise in elderly patients is important for safe recovery. Ask for a referral to a geriatrician or geriatric psychiatrist if the family physician seems uncertain about how to proceed.
Watch for Mental Health Changes
Anxiety and depression often underlie the original reason the benzodiazepine was prescribed. As the drug is tapered, the underlying condition may surface. This is not a sign that the tapering has failed. It is a signal that the underlying condition needs to be treated with a safer, more appropriate method.
When to Seek Immediate Medical Help
If your elderly loved one shows any of the following signs, seek immediate medical attention:
- Sudden confusion or extreme agitation after stopping or missing a dose
- Seizures
- Difficulty breathing
- Loss of consciousness
- Hallucinations or severe disorientation
These are signs of acute benzodiazepine withdrawal or overdose and are medical emergencies. Do not wait and see.
Conclusion
Benzodiazepine addiction in elderly patients is a serious, widespread, and chronically underaddressed problem that affects millions of older adults and the families who care for them. These medications are not inherently evil — used appropriately and for short periods, they serve a real purpose. But the gap between “prescribed” and “appropriate” becomes dangerously wide in the elderly population, where altered metabolism, polypharmacy, and long-term prescribing patterns create the perfect conditions for physical dependence and cognitive harm.
The seven warning signs covered in this article, from memory problems and increased falls to withdrawal symptoms between doses and extreme resistance to tapering, give families a concrete framework for identifying when a problem may exist. The path forward involves honest conversations, informed advocacy with healthcare providers, a supervised and gradual deprescribing process, and support for safer alternatives like CBT and non-addictive medications. Recovery from long-term benzodiazepine dependence in seniors is absolutely possible, and with the right medical support and family involvement, the outcome for your loved one can be meaningfully better.